
A cataract is any opacity in our natural lens. You would think that opacity in the lens will cause visual problems but that is not entirely true. There are many types of cataracts, some affecting your eyesight very slowly but others, much faster. A cataract only needs surgical removal if it affects your eyesight significant enough to interfere with your daily living.
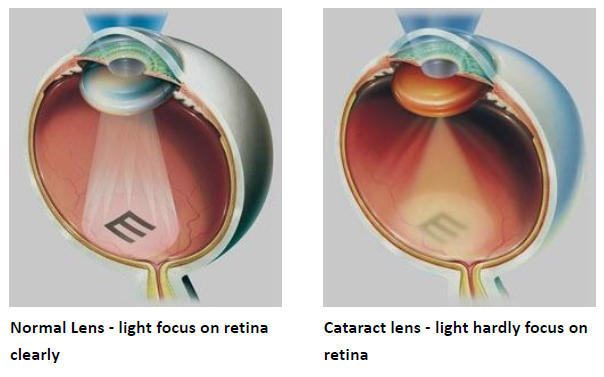
Some cataracts create no symptoms at all. Others lead to worsening nearsightedness or glare. The most common symptom is blurry vision.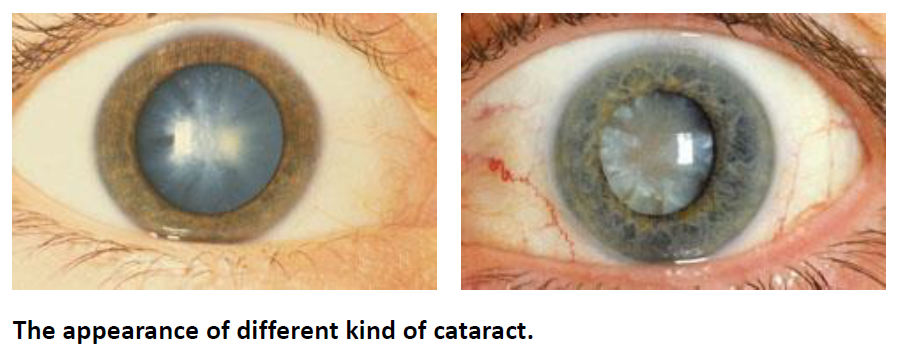
By the time a cataract is matured, an eye's vision is most probably very blurry. Certainly, a matured cataract can still be removed at this stage, but it is also true that removal is more difficult and potentially more hazardous. Corneal edema will be more severe and recovery of vision may take longer. Removal of a visually significant cataract before it reaches the mature stage is now advisable. However, what constitutes “visually significant” is not an unyielding rule. A safe rule of thumb is if your cataract does not bother your eyesight, you do not need to have it removed. If you are in doubt, you should undergo a full examination with your eye doctor. If you are still in doubt, seek more opinion from a different doctor.

"Phacoemulsification" refers to a modern and advanced technique to remove a cataract.
Basically, the central part of the human lens, called the nucleus, is relatively hard and cannot be removed by simple suction like drinking a Cola through a straw.
Therefore in the past, the surgeon would have to make a large opening and then "squeeze out" the nucleus. Having a large opening has several disadvantages. The eye can suddenly bleed profusely during surgery and become blind. A large opening creates potential for large amounts of astigmatism. Most patients undergoing this old type of surgeries need to wear glasses after the surgeries.
In phacoemulsification, the surgeon delivers ultrasound energy through a small probe. The ultrasound energy will convert the hard nucleus into millions of small particles – thus the term “emulsification”. The entire surgery can now be carried out with a very small opening. Visual recovery is relatively faster and patient has less astigmatism. A lot more patients who have undergone phacoemulsification can walk around without the use of eyeglasses.
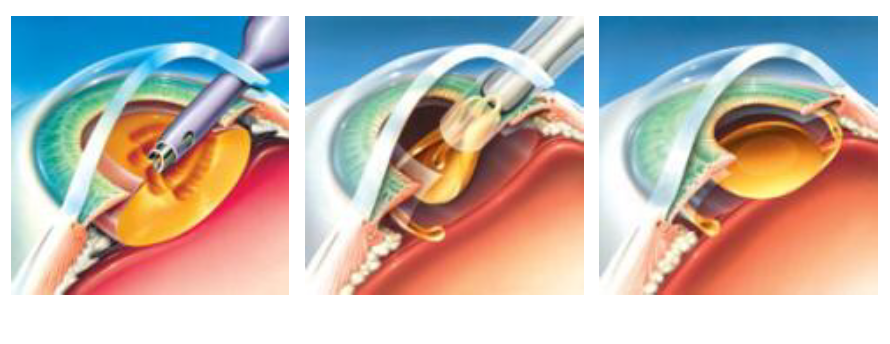
Through a small incision, use a small probe, The ultrasound energy will convert the hard nucleus into millions of small particles and remove them. Insert an intraocular lens & leave it inside the eye
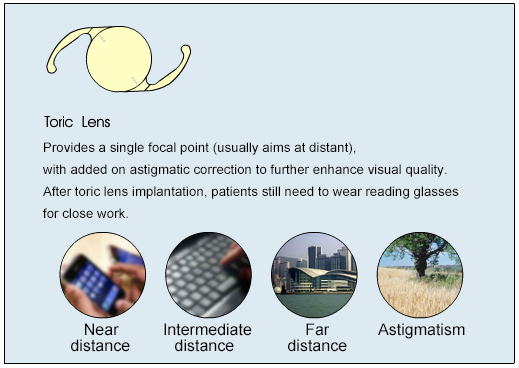
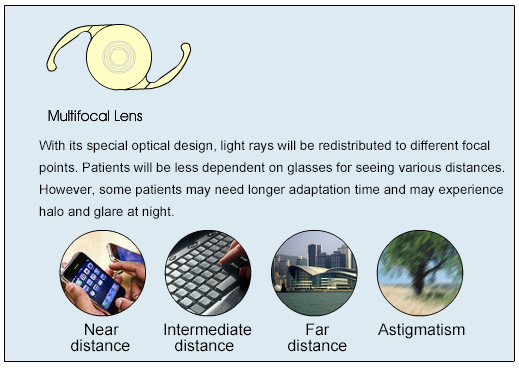
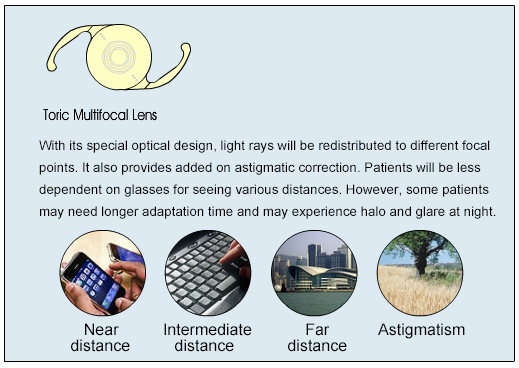
After the surgeon removes a cataract, he usually inserts an intraocular lens. This is a precision-made plastic which replaces the original function of the natural lens – which is to focus light onto the retina

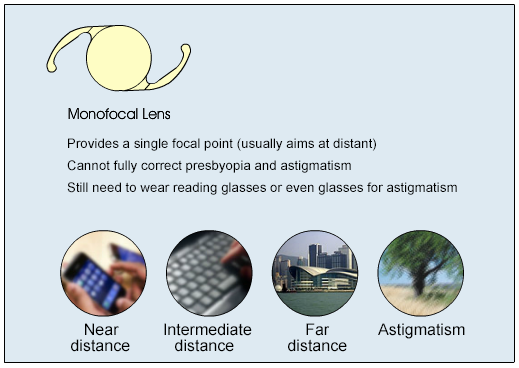
The focal point is elongated by using optical principles, so it provides a longer depth of focus than traditional monofocal intraocular lenses, thus providing better vision at both long and medium distances. It uses smaller optic rings or interval to produce a relatively long focal point, so the halo or glare phenomenon will be less than that of multifocal lenses. Doctors sometimes advocate monovision correction to reduce the patient's dependence on glasses.
